Journal of Cancer
ISSN: 1837-9664
3.2
Impact Factor
ISSN: 1837-9664

 Global reach, higher impact
Global reach, higher impactJ Cancer 2012; 3:113-116. doi:10.7150/jca.4111 This volume Cite
Short Report
All Cancers Age-Adjusted Mortality Rate Surpasses Diseases of the Heart
Stephen W. Wyatt1 ![]() , Hollie R. Sands2, William Ryan Maynard3, Kraig E. Humbaugh4
, Hollie R. Sands2, William Ryan Maynard3, Kraig E. Humbaugh4
1. University of Kentucky, College of Public Health, Lexington, KY, USA;
2. Kentucky Department for Public Health, Frankfort, KY, USA;
3. Louisville, KY, USA;
4. Kentucky Department for Public Health, Frankfort, KY, USA.
Received 2012-1-18; Accepted 2012-2-23; Published 2012-3-3
Citation:
Wyatt SW, Sands HR, Maynard WR, Humbaugh KE. All Cancers Age-Adjusted Mortality Rate Surpasses Diseases of the Heart. J Cancer 2012; 3:113-116. doi:10.7150/jca.4111. https://www.jcancer.org/v03p0113.htm
Other stylesIn 1900, the three leading causes of death in the United States were infectious diseases: Pneumonia/Influenza, Tuberculosis, and Gastritis/Enteritis/Colitis. 1 By the mid-20th century, three chronic diseases (Diseases of the Heart, Malignant Neoplasms and Cerebrovascular Disease) were firmly entrenched as the leading causes of death in the U.S. Late in the 20th century, seven of every ten U.S. resident deaths each year were the result of a chronic disease. At that time, the two most common causes of death, Diseases of the Heart and Malignant Neoplasms (All Cancers) accounted for more than 50% of the total deaths annually in the United States. The number of annual deaths attributed to Diseases of the Heart, and the corresponding mortality rate, were both much higher than the corresponding death count/rate for All Cancers. 2 However, over the past decade, the gap between Diseases of the Heart and All Cancers annual death counts and mortality rates has been closing. Declining Diseases of the Heart deaths and mortality rates- attributed to several factors including: improved access to emergency care for acute events, an enhanced portfolio of medications that reduce risk for heart disease deaths, evolving diagnostic and treatment technologies/strategies, and increased public health interventions- have made monitoring mortality data trends of great public health interest.
Methods
Death data were collected in the Commonwealth of Kentucky using the certificate of death form, and analyzed for the years 2005-2009. Medical certifiers (physicians, coroners, chiropractors, or dentists, by law in Kentucky) were responsible for entering immediate and underlying causes of death. All causes of death are either handwritten or typed by the medical certifier. No electronic death reporting system was available in the state prior to July 2010.
The analysis that we report on was limited to immediate cause of death data. No analyses were conducted on underlying or secondary causes of death. Immediate cause of death is defined as “final disease or condition resulting in death” and underlying cause defined as “disease or injury that initiated events resulting in death.” Due to the exchange of vital records data among states, the analysis included death data from all Kentucky residents, regardless of place of death. Rank order for causes of death was determined by total count of occurrences for a given year.
National Center for Health Statistics (NCHS) mortality coders assigned death codes to each cause of death using the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision. 3 NCHS provides consistent and standard categories for 113 selected causes of death. The NCHS leading causes of death are taken from the list of 113, including the 10 most common which are presented in this report: Diseases of the Heart (I00-I09, I11, I13, I20-I51); Malignant Neoplasms/All Cancers (C00-C97); Cerebrovascular Diseases (I60-I69); Chronic Lower Respiratory Diseases (J40-J47); Alzheimer's Disease (G30); Accidents (Unintentional Injuries) (V01-X59, Y85-Y86); Diabetes Mellitus (E10-E14); Influenza and Pneumonia (J10-J18); Nephritis, Nephrotic Syndrome, Nephrosis (N00-N07, N17-N19, N25-N27); and Septicemia (A40-A41).
Annual state population estimates used to calculate crude mortality rates (CMR) were provided by the Kentucky State Data Center, University of Louisville. The total death counts, CMR, and the Age-Adjusted Mortality Rates (AAR) are important indicators of disease burden within the population. The AAR is an important indicator since it controls for the effect of age in the population, allowing for comparisons over time regarding the influence of factors other than age on death rates. All age-adjusted mortality rates were standardized to the 2000 U.S. population.
Findings
During the five-year period, 2005 to 2009, Diseases of the Heart caused the greatest number of deaths (4,614) among Kentucky female residents, as compared to the 4,515 deaths attributed to All Cancers. However, for the first time the All Cancers age-adjusted mortality rate eclipsed the corresponding Diseases of the Heart rate among female Kentuckians. (Figure 1)
Table 1 presents annual death counts, Crude Mortality Rates (CMR), and Age-Adjusted Mortality Rates (AAR) for both All Cancers and Diseases of the Heart, for Kentucky female residents who died during the 2005-2009 time period. During this five year period, the annual death count, CMR and the AAR for Diseases of the Heart decreased each year. Counts of annual deaths attributed to All Cancers fluctuated over the five-year period, as did the CMR and AAR, but compared to the counts and rates for Diseases of the Heart, remained much more stable. The CMR gap between Diseases of the Heart and All Cancers narrowed considerably during this period. In 2005, the CMR for Diseases of the Heart was 25% higher than the All Cancers CMR; by 2009 the CMR for Diseases of the Heart was only 2% higher.
For female residents of Kentucky, Table 2 presents annual death counts and crude mortality rates for the ten leading causes of death for the most recent five-year period for which data are available. Comparing the first year (2005) and last year (2009) of the 5-year period, three (Diseases of the Heart, Cerebrovascular Diseases, and Influenza/Pneumonia) of the ten leading causes of death exhibited a decrease in the number of annual deaths.
Only Diseases of the Heart deaths decreased in each year of the five-year period. From the 2005 to 2009, Diseases of the Heart exhibited the largest decrease in the number (790 or 14.6%) of deaths. In contrast, Chronic Lower Respiratory Diseases and All Cancers showed the largest increase in the number of deaths; 205 (15.7%) and 195 (4.5%) respectively. Septicemia showed the largest percentage increase (25.2% and 78 deaths).
Figure 1
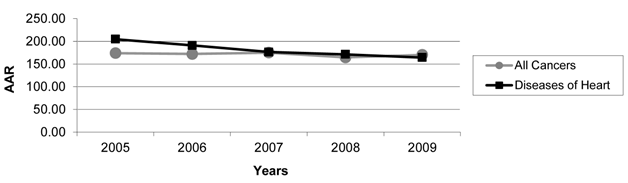
Age-Adjusted Mortality Rates (AAR) For Kentucky Females, 2005-2009
Table 1
Death Counts and Mortality Rates, Kentucky Female Residents, 2005-2009
| 2005 | 2006 | 2007 | 2008 | 2009 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Count | CMR† | AAR‡ | Count | CMR† | AAR‡ | Count | CMR† | AAR‡ | Count | CMR† | AAR‡ | Count | CMR† | AAR‡ | |
| All Cancers | 4,320 | 203.15 | 174.08 | 4,365 | 203.47 | 172.26 | 4,522 | 209.26 | 175.14 | 4,335 | 198.75 | 164.68 | 4,515 | 205.53 | 170.21 |
| Diseases of Heart | 5,404 | 254.13 | 204.87 | 5,144 | 239.78 | 190.95 | 4,842 | 224.07 | 176.44 | 4,837 | 221.77 | 171.37 | 4,614 | 210.04 | 164.24 |
† CMR; Crude Mortality Rate per 100,000
‡ AAR; Age-Adjusted Mortality Rate, per 100,000 of the 2000 US Standard Population
Table 2
Annual Leading Causes of Death of Female Kentuckians, 2005-2009
| 2005 | 2006 | 2007 | 2008 | 2009 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Count | CMR† | Count | CMR† | Count | CMR† | Count | CMR† | Count | CMR† | |
| DISEASES OF HEART | 5,404 | 254.13 | 5,144 | 239.78 | 4,842 | 224.07 | 4,837 | 221.77 | 4,614 | 210.04 |
| ALL CANCERS | 4,320 | 203.15 | 4,365 | 203.47 | 4,522 | 209.26 | 4,335 | 198.75 | 4,515 | 205.53 |
| CEREBROVASCULAR DISEASES | 1,313 | 61.75 | 1,301 | 60.64 | 1,326 | 61.36 | 1,231 | 56.44 | 1,211 | 55.13 |
| CHRONIC LOWER RESPIRATORY DISEASES | 1,303 | 61.28 | 1,236 | 57.61 | 1,328 | 61.45 | 1,488 | 68.22 | 1,508 | 68.65 |
| ALZHEIMER'S DISEASE | 836 | 39.31 | 823 | 38.36 | 858 | 39.70 | 986 | 45.21 | 948 | 43.16 |
| ACCIDENTS (UNINTENTIONAL INJURIES) | 751 | 35.32 | 831 | 38.74 | 781 | 36.14 | 833 | 38.19 | 803 | 36.55 |
| DIABETES MELLITUS | 650 | 30.57 | 594 | 27.69 | 521 | 24.11 | 609 | 27.92 | 668 | 30.41 |
| INFLUENZA AND PNEUMONIA | 584 | 27.46 | 492 | 22.93 | 497 | 23.00 | 504 | 23.11 | 543 | 24.72 |
| NEPHRITIS, NEPHROTIC SYNDROME AND NEPHROSIS | 472 | 22.20 | 482 | 22.47 | 520 | 24.06 | 516 | 23.66 | 478 | 21.76 |
| SEPTICEMIA | 309 | 14.53 | 354 | 16.50 | 366 | 16.94 | 379 | 17.38 | 387 | 17.62 |
† CMR; Crude Mortality Rate, per 100,000
Discussion
The finding that the All Cancers age-adjusted mortality rate surpassed the corresponding rate for Diseases of the Heart among female Kentucky residents in 2009 is both significant and historic. A companion analysis for males in Kentucky, for the same time period, did not demonstrate a similar “crossing-over” of age-adjusted mortality rate trend lines for the two leading causes of death among Kentucky males, although the gap narrowed considerably. In addition, an analysis of All Cancers and the broader classification of Cardiovascular Diseases mortality among Kentucky females over the same time period, showed that the AAR gap narrowed considerably as well. In 2005, the Cardiovascular Diseases AAR among females in Kentucky was 57% higher than the All Cancers AAR; by 2009 it was only 31% higher.
The trend line (Figure 1) shows that the crossover occurred because the Diseases of the Heart AAR declined during the 5-year period, while the All Cancers AAR remained relatively stable. In addition to the factors previously cited as contributing to the declining mortality from Diseases of the Heart, smoking is an established risk factor for both heart disease and several cancers. In a state where smoking prevalence is high, this is an important issue. Although the prevalence of smoking among Kentucky adults is consistently among the highest in the U.S., adult smoking prevalence has decreased over the past decade due to enhanced public health interventions, including health policy efforts. 4 It is reasonable to argue that these reductions in adult smoking prevalence would impact Diseases of the Heart mortality much sooner than the All Cancers mortality. As with most analyses there are limitations. The primary limitation of the analysis is related to the reliance upon the accuracy and completeness of death certificate information/data.
The steady decline in Diseases of the Heart deaths, and associated mortality rates is a true success story. In their textbook, The New Public Health, Tulchchinsky and Varavikova state: “The most important lesson since the 1950's in public health is that these (Heart Disease) risk factors and diseases can be reduced dramatically by suitable public health interventions.” 5 While many public health leaders likely can/would argue that the decline in cervical cancer mortality, since the introduction of the Papanicolaou Smear in the 1950's, is one of the most compelling “lessons-learned” in public health, it is not debatable that efforts to reduce heart disease risk factors and the subsequent decline in mortality is an impressive public health success story.
Acknowledgements
Paul F. Royce, Kentucky Department for Public Health. Steve Davis, Kentucky Department for Public Health. Jessica Jones, University of Kentucky, College of Public Health.
Conflict of Interest
The authors have declared that no conflict of interest exists.
References
1. Brownson RC, Remington PL, Davis JR. Chronic Disease Epidemiology and Control. American Public Health Association. 1998
2. Centers for Disease Control and Prevention. Indicators for Chronic Disease Surveillance. MMWR. 2004;53:1-6
3. World Health Organization. International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Volume 2, Second Edition. WHO. 1992: 1.
4. Accessed 01/18/2012. Kentucky Health Facts; Foundation for a Healthy Kentucky. http://Kentuckyhealthfacts.org
5. Tulchinsky TH, Varavikova EA. What is the “New Public Health”? Public Health Reviews. 2010;32:25-53
Author contact
![]() Corresponding author: swwyat2uky.edu
Corresponding author: swwyat2uky.edu
Citation styles
APA
Wyatt, S.W., Sands, H.R., Maynard, W.R., Humbaugh, K.E. (2012). All Cancers Age-Adjusted Mortality Rate Surpasses Diseases of the Heart. Journal of Cancer, 3, 113-116. https://doi.org/10.7150/jca.4111.
ACS
Wyatt, S.W.; Sands, H.R.; Maynard, W.R.; Humbaugh, K.E. All Cancers Age-Adjusted Mortality Rate Surpasses Diseases of the Heart. J. Cancer 2012, 3, 113-116. DOI: 10.7150/jca.4111.
NLM
Wyatt SW, Sands HR, Maynard WR, Humbaugh KE. All Cancers Age-Adjusted Mortality Rate Surpasses Diseases of the Heart. J Cancer 2012; 3:113-116. doi:10.7150/jca.4111. https://www.jcancer.org/v03p0113.htm
CSE
Wyatt SW, Sands HR, Maynard WR, Humbaugh KE. 2012. All Cancers Age-Adjusted Mortality Rate Surpasses Diseases of the Heart. J Cancer. 3:113-116.
This is an open access article distributed under the terms of the Creative Commons Attribution (CC BY-NC) License. See http://ivyspring.com/terms for full terms and conditions.