Impact Factor ISSN: 1837-9664

 Global reach, higher impact
Global reach, higher impactJ Cancer 2026; 17(6):1220-1228. doi:10.7150/jca.133473 This issue Cite
Research Paper
GALNT14-rs9679162 Genotypes Predict Post-immunotherapy Side Effect and Survival in Patients with Hepatitis B Virus-related Hepatocellular Carcinoma
Po-Ting Lin1,2,3, Wei Teng1,2, Wei-Ting Chen1,2,4, Yu-De Chu4, Chung-Wei Su1,2, Yi-Chung Hsieh1,2, Chen-Chun Lin2,5, Yung-Chang Lin2,6, Chun-Yen Lin1,2, ![]() , Chau-Ting Yeh1,2,4,7,
, Chau-Ting Yeh1,2,4,7, ![]() , Shi-Ming Lin1,2
, Shi-Ming Lin1,2
1. Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou branch, No. 5, Fuxing St., Guishan Dist., Taoyuan City, 333, Taiwan.
2. College of Medicine, Chang Gung University, No.259, Wenhua 1st Rd., Guishan Dist., Taoyuan City 333, Taiwan.
3. Graduate Institute of Clinical Medical Sciences, College of Medicine, Chang Gung University, No.259, Wenhua 1st Rd., Guishan Dist., Taoyuan City 333, Taiwan.
4. Liver Research Center, Linkou Chang Gung Memorial Hospital, No. 5, Fuxing St., Guishan Dist., Taoyuan City, 333, Taiwan.
5. Department of Gastroenterology and Hepatology, New Taipei Municipal Tucheng Hospital, No.6, Sec.2, Jincheng Rd., Tucheng Dist., New Taipei City 236, Taiwan.
6. Department of Hematology-Oncology, Chang Gung Memorial Hospital, Linkou branch, No. 5, Fuxing St., Guishan Dist., Taoyuan City, 333, Taiwan.
7. Institute of Stem Cell and Translational Cancer Research, Linkou Chang Gung Memorial Hospital, No. 5, Fuxing St., Guishan Dist., Taoyuan City, 333, Taiwan.
* These authors contributed equally to this work as corresponding authors.
Received 2026-2-24; Accepted 2026-6-2; Published 2026-6-10
Abstract

Introduction: Genomic alterations have been reported to correlate with patients' response to immune checkpoint inhibitor (ICI) therapy in hepatocellular carcinoma (HCC). The present study aimed to examine whether single nucleotide polymorphism (SNP) is associated with ICI treatment-related side effects and progression-free survival (PFS) in HCC patients.
Methods: This retrospective study included 96 patients with HBV-related HCC receiving ICI (atezolizumab plus bevazizumab) therapy between 2020 and 2023. Five SNPs derived from a previous genome-wide association study linking to chemotherapy responses in HCC patients were included. Their predictive values for PFS and side effects were examined.
Results: After ICI therapy, patients with GALNT14-rs9679162 “GG” genotype (median PFS = 19.7 months, 95% confidence interval [CI]: 12.3-35.7; p = 0.032) had a longer PFS, whereas GALNT14-rs675230, BMP7-rs6025211, WWOX-rs13338697 or WWOX-rs13333314 were not associated with PFS (all p > 0.05). GALNT14-rs9679162 “GG” genotype (odds ratio [OR] = 0.298, 95% CI: 0.096-0.926; p = 0.036) was also associated with a decreased risk of post-treatment high-grade aspartate aminotransferase (AST) elevation. Multivariate analysis showed that GALNT14-rs9679162 “GG” genotype (hazard ratio [HR] = 0.433, 95% CI: 0.212-0.886; p = 0.022) and high initial albumin-bilirubin (ALBI) grade (HR = 2.053, 95% CI: 1.153-3.590; p = 0.014) were independently associated with PFS.
Conclusions: Genetic variant of an SNP, GALNT14-rs9679162, predicts post-treatment PFS and side effect in HBV-related HCC patients receiving ICIs therapy.
Keywords: hepatocellular carcinoma (HCC), progression-free survival (PFS), rs6752303, side effects, single nucleotide polymorphism (SNP)
Introduction
Hepatocellular carcinoma (HCC), the third leading cause of cancer-related deaths in the world, has been referred to as a highly devastating malignancy, with a low 5-year survival rate of about 18% [1]. Although the management of HCC has significantly changed over the last few years owing to improved patient stratification and introduction of novel therapies, it remains debatable regarding which treatment should be considered as 'standard therapy' for HCC cases [2].
The immune checkpoint inhibitors (ICIs), including atezolizumab and bevacizumab, are currently being used as the first-line therapy in patients with HCC [3]. Fin et al. [4] have revealed that atezolizumab combined with bevacizumab results in better overall and progression-free survival (PFS) outcomes than sorafenib in unresectable HCC. However, despite the encouraging results, immunotherapy does not guarantee a clinical benefit in all patients with HCC, and more than two-thirds of advanced stage patients do not respond to immunotherapy [5]. In addition, although the toxicity profile of the ICIs (anti-PD-1 agents) seems favorable with about 10% of patients experiencing grade 3-4 adverse events, the risk of immune-mediated toxicities warrants strict vigilance concerning symptoms of colitis, pneumonitis, and especially hepatitis in patients with HCC [6].
A previous genome-wide association study attempting to identified SNPs linking to chemotherapeutic responses in advanced HCC has resulted in discovery of a few predictive markers. Of the two single nucleotide polymorphisms (SNPs) rs9679162 and rs6752303 flanking GALNT14, the TT genotype of GALNT14-rs9679162 was found to be a reliable marker for therapeutic outcome in advanced HCC patients treated with chemotherapy [7] or sorafenib [8]. WWOX SNP (rs13338697) predicted the therapeutic efficacy of ADI-PEG 20 in patients with advanced HCC [9]. A previous study reports that patients with HCC carrying the GALNT14-rs9679162 TT genotype have lower GALNT14 expression and favorable prognosis [10]. They suggest that overexpression of GALNT14 may enhance hepatocarcinogenesis/progression and resistance to anticancer drugs via O-glycosylation at Ser161 of prohibitin-2 (PHB2) in the endoplasmic reticulum and/or cell membrane. Furthermore, GALNT14 genetic variants are correlated to HCC postoperative prognosis, and GALNT14 expression is associated with abundance of M2-macrophages in tumor microenvironment [11]. A recent study indicates that patients with HBV-related HCC show better responses to immunotherapy [12]. However, no study has currently investigated whether these SNPs are associated with ICI-related responses in HBV-positive advanced HCC patients. Further understanding of the genomic background of HCC is essential to overcome therapeutic challenges of ICIs so that clinicians can carefully select favorable patients to receive ICI therapy and, to advise unfavorable patients to choose other novel effective treatments. Therefore, the present study aimed to further determine the associations between these SNPs and ICI treatment-related side effects and survival in patients with HBV-related HCC.
Materials and Methods
Study design and patient selection
This retrospective study reviewed patients with HCC receiving ICIs (atezolizumab plus bevazizumab) therapy between 2020 and 2023. Exclusion criteria were: 1) Patients without HBV; 2) ICI treatment < 3 cycles; 3) No post-treatment image; 4) Curative HCC; and 5) Double cancers. After exclusion, 96 patients were included in the analysis (Figure S1).
Baseline demographic and clinical data collected from the medical records were age, sex, BCLC classification, microvascular invasion (MVI), portal vein invasion (VP) stage, up to 7 criteria [13], or up to 11 criteria [14], extra-hepatic metastasis (EHM), treatment with transarterial chemoembolization (TACE) and/or radiofrequency ablation (RFA), history of hepatitis B virus (HBV), neutrophil-to-lymphocyte ratio (NLR), platelets, albumin, alpha fetoprotein (AFP), γ-GT, alanine transaminase (ALT), albumin-bilirubin (ALBI) grade, and previous gastrointestinal drug. Patients were followed with hepatic ultrasonography and computed tomography (CT) every 3-6 months, and serum AFP and serum protein levels were assessed every month; these data were also extracted from the medical records.
Main outcome measures assessment
Primary outcomes included overall survival (OS), PFS, treatment response, objective response rate (ORR), disease control rate (DCR) and a decrease of serum AFP of 20% from baseline in patients with ICI. The secondary outcomes were to determine the factors associated with post-treatment OS or post-treatment PFS. Treatment response evaluation was based on the modified Response Evaluation Criteria in Solid Tumors (mRECIST) [15]. ORR was defined as the percentage of patients who achieve a response, which was either be complete response (CR; complete disappearance of lesions) or partial response (PR; reduction in the sum of maximal tumor diameters by at least 30%) [15]. The DCR was defined as the percentage of patients who achieved a CR, PR, and stable disease, as reported previously [16]. The OS rate was defined as the interval between ICI treatment and the date of death caused by HCC or the date of the last follow-up. PFS was defined as the interval between ICI therapy and the date of diagnosis of the first recurrence or the date of the last follow-up.
Ethical considerations
The study protocol was approved by the Institutional Review Board (IRB) of our hospital (Approval number: 20240041B0) and was conducted in accordance with both the Declarations of Helsinki and Istanbul. In addition, the need for patients' informed consent was waived by the IRB because the study was as retrospective cross-sectional, observational study with expedited review. All medical records of patients diagnosed with HCC treated with the ICIs between 2020 and 2023 were reviewed (Figure S1).
SNP genotyping
The genotyping of the SNPs was conducted following previously established procedures [10]. In brief, genomic DNA isolated from blood samples was extracted using the QIAamp DNA mini kit (QIAGEN, Hilton, Germany), adhering to the manufacturer's provided instructions. Semi-nested polymerase chain reaction (PCR) was performed with the following primers: GALNT14-F1: 5'-TCACGAGGCCAACATTCTAG-3'; GALNT14-R1: 5'-TTAGA-TTCTGCATGGCTCAC-3'; GALNT14-R2: 5'-TCCCTCCTACTGAACCTCTCC-3'; WWOX-F1: 5'-ACTTCTGACAGCCATCCAGA-3'; WWOX-F2: 5'-ATCCTGCTAGCATGTTGACT-3'; WWOX-R2: 5'-ACTGTAGATGCCTTCCATCT-3'; Rs6025211-F1: 5'-ACATTCACAGAGAACTTGGC-3'; Rs6025211-R1: 5'-CAAGCAGTCCTTCCACCTTG-3'; Rs6025211-R2: 5'-AAAGTGCTGGGATTACAGG-T-3'. The amplified PCR products underwent gel purification using the EasyPrep Gel & PCR Extraction Kit (BIOTOOLS, New Taipei City, Taiwan).
Side effects evaluation
Side effects were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
Statistical analysis
Continuous variables were expressed as medians with corresponding range or 95% confidence interval (CI), and compared using Mann-Whitney U test. Categorical variables were expressed as number and percentage, and are compared using Fisher's exact test. The Kaplan-Meier method was used to compare survival times between the two genotypes, and survival curves were compared using the log-rank test. Cox regression analysis was performed to determine associations between demographic and clinical variables and PFS of patients with each genotype. Time-to-event was defined as “the follow-up period of event occurrence”. Logistic regression analysis was performed to determine associations between patients' demographic and clinical variables and post-treatment aspartate aminotransferase (AST) grade. A 2-sided value of p < 0.05 was established as statistical significance. Statistical analyses were performed using SPSS version 25.0 software (SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics
The demographic and clinical characteristics of 96 patients with HCC are shown in Table 1, including 81 (84,4%) males and 15 (15.6%) females, with median age 60.7 (33.3-83.1) years. Median baseline scores for NLR, platelets, albumin, AFP, γ-GT and ALP were 3.9 (1.4-51.4), 176.0 (39.0-750.0) 103/μL, 3.8 (2.5-4.7) g/dL, 371.0 (2.0-211754.9) ng/mL, 127.0 (19.0-768.0) U/L and 119.0 (44.0-1283.0) U/L, respectively. The relative majority were BCLC stage C (74.0%), no MVI (51.0%), up-to-7 criteria (78.1%), up-to-11 criteria (57.3%), no EHM (53.1%), previous TACE (53.1%), no previous RFA (71.9%), history of HBV (100%), ALBI II or III (63.5%), and no previous GI drugs (83.3%). In addition, 23 (24%) patients were rs6752303 with TT genotype, 21 (21.9%) patients were GALNT14-rs9679162 with GG genotype, 14 (14.6%) patients were rs6025211 with TT genotype, 9 (9.4%) patients were rs13338697 with GG genotype, and 9 (9.4%) patients were rs13333314 with AA genotype.
Patients' baseline demographic and clinical characteristics
| Variables | Patients (n = 96) |
|---|---|
| Age (years), median (range) | 60.7 (33.3-83.1) |
| Sex/male, n (%) | 81 (84.4) |
| BCLC stage, n (%) | |
| A | 6 (6.3) |
| B | 19 (19.8) |
| C | 71 (74.0) |
| MVI, n (%) | 47 (49.0) |
| VP stage, n (%) | |
| VP2 | 3 (6.4) |
| VP3 | 26 (55.3) |
| VP4 | 18 (38.3) |
| Out of up-to-7 criteria, n (%) | 75 (78.1) |
| Out of up-to-11 criteria, n (%) | 55 (57.3) |
| EHM, n (%) | 45 (46.9) |
| Prior LRT, n (%) | |
| TACE | 51 (53.1) |
| RFA | 27 (28.1) |
| Prior TKI, n (%) | 40 (41.7) |
| HBV history, n (%) | 96 (100.0) |
| Baseline NLR, median (range) | 3.9 (1.4-51.4) |
| Baseline platelets (103/μL), median (range) | 176.0 (39.0-750.0) |
| Baseline albumin (g/dL), median (range) | 3.8 (2.5-4.7) |
| Baseline AFP (ng/mL), median (range) | 371.0 (2.0-211754.9) |
| Baseline γ-GT (U/L), median (range) | 127.0 (19.0-768.0) |
| Baseline ALP (U/L), median (range) | 119.0 (44.0-1283.0) |
| Baseline ALBI II+III, n (%) | 61 (63.5) |
| Previous gastrointestinal drug, n (%) | 16 (16.7) |
| GALNT14-rs9679162, n (%) | |
| Non-GG | 75 (78.1) |
| GG | 21 (21.9) |
| GALNT14-rs6752303, n (%) | |
| Non-TT | 73 (76.0) |
| TT | 23 (24.0) |
| BMP7-rs6025211, n (%) | |
| Non-TT | 82 (85.4) |
| TT | 14 (14.6) |
| WWOX-rs13338697, n (%) | |
| Non-GG | 87 (90.6) |
| GG | 9 (9.4) |
| WWOX-rs13333314, n (%) | |
| Non-AA | 87 (90.6) |
| AA | 9 (9.4) |
Abbreviations: ICI, immune checkpoint inhibitor; BCLC; Barcelona Clinic Liver Cancer classification; MVI, microvascular invasion; VP, portal vein invasion; EHM, extra-hepatic metastasis; TACE, transarterial chemoembolization; RFA, radiofrequency ablation; HBV, hepatitis B virus; NLR, neutrophil-to-lymphocyte ratio; AST, aspartate aminotransferase; ALT, alanine transaminase; AFP, alpha fetoprotein; ALBI grade, albumin-bilirubin grade; APRI, aspartate aminotransferase to platelet ratio index; FIB-4, fibrosis-4 index; LRT, locoregional therapy; IQR, interquartile range. aTransarterial chemoembolization or radiofrequency ablation. *p < 0.05.
Outcomes between the two genotypes
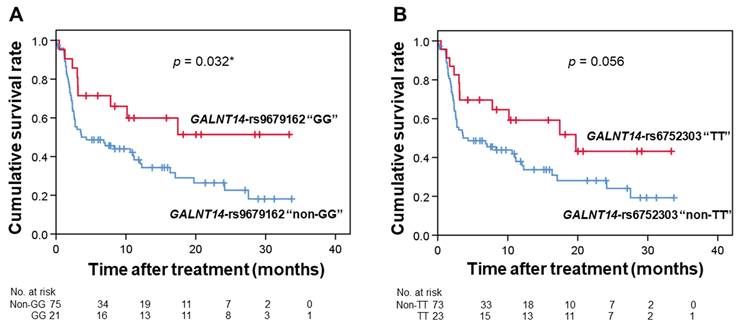
After treatment, the median follow-up period in GALNT14-rs9679162 with GG and non-GG was 10.4 (1.4 ± 33.4) months and 7.8 (0.1-33.8) months, respectively (p > 0.05, Table 2). Patient with GG genotype had a higher median PFS than patients with non-GG genotype (GG vs non-GG genotypes: 19.7 [12.3-35.7] vs 4.3 [0-9.9] months; p = 0.032, Table 2 and Figure 1A). Moreover, disease control rate slightly increased in patients with GG genotype (71.4%) when compared with those with non-GG genotype (50.7%) (p = 0.136, Table 2). During a similar median follow-up period, GALNT14-rs6752303 with TT also had a higher PFS than GALNT14-rs9679162 with non-TT, although it was not statistically different (TT vs. non-TT genotypes: 19.7 [5.2-34.3] vs 4.3 [0-9.8] months, p=0.056, Table 2 and Figure 1B). Compared to patients with non-TT genotype (50.7%), disease control rate also slightly increased in patients GG genotype (69.6%) (p = 0.150, Table 2). In contrast, PFS and disease control rate were not significantly different between the genotypes of BMP7-rs6025211, WWOX-rs13338697 or WWOX-rs13333314 (all p > 0.05, Table S1).
Patients' response and outcome assessment for immune therapy between the two genotypes.
| GALNT14- rs9679162 | GALNT14-rs6752303 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Review according to mRECIST | Non-GG (n = 75) | GG (n = 21) | p-value | Non-TT (n = 73) | TT (n = 23) | p-value | ||||
| AFP decrease 20% from baselinea, n (%) | 20 (26.7) | 7 (33.3) | 0.588 | 20 (27.4) | 7 (30.4) | 0.794 | ||||
| Treatment response, n (%) | 0.210 | 0.166 | ||||||||
| Complete response | 0 (0) | (0) | 0 (0) | (0) | ||||||
| Partial response | 15 (20.0) | 5 (23.8) | 15 (20.5) | 5 (21.7) | ||||||
| Stable disease | 23 (30.7) | 10 (47.6) | 22 (30.1) | 11 (47.8) | ||||||
| Progressive disease | 27 (36.0) | 6 (28.6) | 26 (35.6) | 7 (30.4) | ||||||
| Not evaluable | 10 (13.3) | 0 (0) | 10 (13.7) | 0 (0) | ||||||
| Objective response rate, n (%) | 15 (20.0) | 5 (23.8) | 0.763 | 15 (20.5) | 5 (21.7) | 1.000 | ||||
| Disease control rate, n (%) | 38 (50.7) | 15 (71.4) | 0.136 | 37 (50.7) | 16 (69.6) | 0.150 | ||||
| Follow up duration (months), median (range) | 7.8 (0.1, 34.77) | 10.4 (1.4, 33.4) | 0.158 | 7.8 (0.1, 34.77) | 10.4 (1.4, 33.4) | 0.158 | ||||
| Overall survival (months), median (95% CI) | 12.3 (7.2-17.3) | 17.4 (4.4-32.8) | 0.245 | 12.3 (10.0, 14.5) | 17.4 (3.6, 31.2) | 0.392 | ||||
| Progression-free survival (months), median (95% CI) | 4.3 (0-9.9) | 19.7 (12.3-35.7) | 0.032* | 4.3 (0, 9.8) | 19.7 (5.2, 34.3) | 0.056 | ||||
Abbreviations: mRECIST, modified Response Evaluation Criteria in Solid Tumors; AFP, alpha fetoprotein. aPatients with a baseline AFP level < 10 were excluded from AFP decrease by 20% analysis.
Kaplan-Meier survival curves for HCC patients. Kaplan-Meier survival curves for 96 HCC patients stratified by GALNT14-rs9679162 (A) and GALNT14-rs6752303 (B). *p<0.05.
Associations between genotype and post-treatment side effects
Compared to GALNT14-rs9679162 with the non-GG genotype, GALNT14-rs9679162 with GG genotype had a higher proportion of post-treatment AST with a low grade (p = 0.034, Table S2). However, the distribution of other post-treatment side effects, including ALT, hypertension, proteinuria, hyperthyroidism, hypothyroidism, rash, fatigue, dizziness, myalgia, pruritus, diarrhea, HFSR, edema, fever, pneumonitis, colitis, abdominal pain, vomiting or nausea, GI bleeding, and GI bleeding prevention, was not significantly different between the two genotype groups (all p > 0.05, Table S2). Similarly, GALNT14 rs6752303 with TT genotype had a higher proportion of post-treatment AST with a low grade (p = 0.010, Table S2).
Subsequent multivariate logistic regression analysis showed that GALNT14-rs9679162 with GG (odds ratio [OR] = 0.298, 95% CI: 0.096-0.926; p = 0.036) was associated with a decreased risk of post-treatment AST high grade elevation (Table 3). However, age, sex, BCLC stage, MVI, out-to-7 criteria, EHM, and ALBI grade were not significantly associated with post-treatment AST grade (all p > 0.05, Table 3). Similarly, GALNT14 rs6752303 with TT (OR = 0.236, 95% CI: 0.077-0.721; p = 0.011) was associated with a decreased risk of post-treatment AST high grade elevation (Table S3).
Univariate and multivariate logistic regression analyses of post-treatment AST grade
| Variables | Number | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |||
| Sex | Female | 15 | Ref. | Ref. | ||
| Male | 81 | 0.673 (0.419, 3.852) | 0.673 | 0.703 (0.224, 2.205) | 0.546 | |
| Age | 96 | 0.985 (0.949, 1.023) | 0.436 | 0.990 (0.953, 1.028) | 0.591 | |
| GALNT14_rs9679162 | Non-GG | 75 | Ref. | Ref. | ||
| GG | 21 | 0.284 (0.092, 0.880) | 0.029* | 0.298 (0.096, 0.926) | 0.036* | |
| BCLC stage | A | 6 | Ref. | |||
| B | 19 | 7.857 (0.452, 82.128) | 0.185 | |||
| C | 71 | 5.469 (0.606, 49.351) | 0.130 | |||
| MVI | No | 49 | Ref. | |||
| Yes | 47 | 0.737 (0.323, 1.683) | 0.469 | |||
| Out of up-to-7 criteria | No | 21 | Ref. | |||
| Yes | 75 | 1.583 (0.592, 4.235) | 0.360 | |||
| EHM | No | 51 | Ref. | |||
| Yes | 45 | 1.495 (0.654, 3.419) | 0.340 | |||
| Prior LRT | No | 40 | Ref. | |||
| Yes | 56 | 0.530 (0.226, 1.247) | 0.146 | |||
| Prior TKI | No | 56 | Ref. | |||
| Yes | 40 | 0.844 (0.367, 1.946) | 0.691 | |||
| ALBI | I | 35 | Ref. | |||
| II+III | 61 | 0.545 (0.228, 1.303) | 0.172 | |||
| AFP drop 20% from baseline | No | 69 | Ref. | |||
| Yes | 27 | 0.684 (0.236, 1.982) | 0.484 |
AST, aspartate amino transferase; BCLC; Barcelona Clinic Liver Cancer classification; MVI, microvascular invasion; EHM, extra-hepatic metastasis; LRT, loco-regional therapy; TKI, tyrosine kinase inhibitor; ALBI grade, albumin-bilirubin grade; AFP, alpha fetoprotein; OR, odds ratio; CI, confidence interval. *p < 0.05.
Factors associated with post-treatment PFS
In the multivariate Cox regression analysis, GALNT14-rs9679162 with GG (hazard ratio [HR] = 0.433, 95% confidence interval [CI]: 0.212-0.886; p = 0.022) was associated with a decreased risk of post-treatment disease progression, while ALBI grade II/III (HR = 2.053, 95% CI: 1.153-3.590; p = 0.014) was significantly associated with an increased risk of post-treatment disease progression (Table 4). However, sex, BCLC stage, MVI, out-to-7 criteria, out-to-11 criteria, EHM, 20% improvement of AFP, line of ICI treatment, post-treatment AST grade, and post-treatment HFSR grade were not significantly associated with post-treatment disease progression (all p > 0.05, Table 4).
Univariate and multivariate Cox regression analyses of post-treatment disease progression.
| Variables | Number | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p-value | HR (95% CI) | p-value | |||
| Sex | Female | 15 | Ref. | Ref. | ||
| Male | 81 | 0.654 (0.336, 1.273) | 0.211 | 0.821 (0.418, 1.612) | 0.566 | |
| Age | 96 | 0.976 (0.954, 0.997) | 0.040* | 0.979 (0.956, 0.999) | 0.048* | |
| GALNT14_ rs9679162 | Non-GG | 75 | Ref. | |||
| GG | 21 | 0.468 (0.230, 0.952) | 0.036* | 0.433 (0.212, 0.886) | 0.022* | |
| BCLC stage | A | 6 | Ref. | |||
| B | 19 | 2.631 (0.578, 11.967) | 0.211 | |||
| C | 71 | 2.845 (0.688, 11.758) | 0.149 | |||
| MVI | No | 49 | Ref. | |||
| Yes | 47 | 1.310 (0.787, 2.181) | 0.298 | |||
| Out of up-to-7 criteria | No | 21 | Ref. | |||
| Yes | 75 | 1.407 (0.745, 2.654) | 0.292 | |||
| EHM | No | 51 | Ref. | |||
| Yes | 45 | 1.010 (0.608, 1.678) | 0.969 | |||
| Prior LRT | No | 40 | Ref. | |||
| Yes | 56 | 0.970 (0.582, 1.617) | 0.907 | |||
| Prior TKI | No | 56 | Ref. | |||
| Yes | 40 | 1.375 (0.824, 2.293) | 0.233 | |||
| ALBI | I | 35 | Ref. | Ref. | ||
| II+III | 61 | 1.913 (1.087, 3.368) | 0.025* | 2.053 (1.153, 3.590) | 0.014* |
AST, aspartate amino transferase; BCLC; Barcelona Clinic Liver Cancer classification; MVI, microvascular invasion; EHM, extra-hepatic metastasis; ALBI grade, albumin-bilirubin grade; AFP, alpha fetoprotein; OR, odds ratio; CI, confidence interval. *p < 0.05.
Side effects are associated with SNP GALNT14-rs9679162-affected post-treatment PFS
To determine whether GALNT14-rs9679162-related post-treatment AST involves in GALNT14-rs9679162-afftected post-treatment disease progression, we further evaluated the association between GALNT14-rs9679162 genotypes and post-treatment disease progression in different AST subgroups (grade 0 and grade ≥ 1) (Table 5). In low AST grade (grade 0) subgroup, multivariate Cox analysis showed that GALNT14-rs9679162 with GG genotype (HR = 0.350, 95% CI: 0.132-0.929; p = 0.035) was associated with a decreased risk of post-treatment disease progression; however, this association was not observed in high AST grade (grade ≥ 1) subgroup (p > 0.05). This indicated that post-treatment AST grade may be associated with GALNT14-rs9679162-related post-treatment disease progression.
Multivariate Cox regression analyses of post-treatment disease progression after stratifying for AST grade.
| Variables | Grade 0 | p-value | Grade ≥ 1 | p-value |
|---|---|---|---|---|
| HR (95% CI) | HR (95% CI) | |||
| Age | 0.996 (0.961, 1.032) | 0.827 | 0.968 (0.936, 1.002) | 0.065 |
| GALNT14_rs9679162 | ||||
| Non-GG | Ref. | |||
| GG | 0.350 (0.132, 0.929) | 0.035* | 0.359 (0.046, 2.779) | 0.327 |
| ALBI | ||||
| I | Ref. | Ref. | ||
| II+III | 1.711 (0.732, 3.999) | 0.215 | 2.523 (1.122, 5.672) | 0.025* |
AST, aspartate amino transferase; ALBI grade, albumin-bilirubin grade; AFP, alpha fetoprotein; HR, hazards ratio; CI, confidence interval. *p < 0.05.
In high AST grade subgroup, multivariate Cox analysis showed that high ALBI grade (grade II and III) (HR = 2.523, 95% CI: 1.122-5.672; p = 0.025) was associated with an increased risk of post-treatment disease progression; however, this association was not observed in low AST grade subgroup (p > 0.05). This indicated that post-treatment AST grade may be also associated with ALBI grade-related post-treatment disease progression.
Discussion
The new key findings of the study included: 1) The GALNT14-rs9679162 “GG” genotype had a longer post-treatment PFS than did GALNT14-rs9679162 “non-GG” genotype in HBV-related HCC patients with ICIs; 2) The GALNT14-rs9679162 “GG” genotype was associated with a decreased risk of post-treatment AST high grade elevation; and 3) The severity of post-treatment AST grade is associated with GALNT14-rs9679162 SNP-affected post-treatment disease progression.
Despite the limited information on the GALNT14-rs9679162 genotype, existing data suggests that this SNP is located within the intron of the GALNT14 gene [17]. SNP GALNT14-rs9679162 has been identified as a reliable indicator for a positive response to chemotherapy [7] or sorafenib [8] treatment in advanced HCC patients. According to the SNP findings in the present study, the frequency of the GALNT14-rs9679162 “GG” genotype in our population with HCC treated with ICIs (n = 96) was approximately 22.9%. In the present study, the GALNT14-rs9679162 genotype could predict a longer PFS following treatment with ICIs in HCC patients. Specifically, individuals with the GALNT14-rs967962 “GG” genotype exhibited a decreased risk of disease progression post-treatment with ICIs compared to those with the “non-GG” genotype. It has been shown that SNPs could modulate several cellular functions through alteration of mRNA secondary structure, modulation of RNA alternative splicing, and regulation of target-gene-translation efficiency [18]. The GALNT14 expression is significantly associated with the adverse survival of patients with HCC [19]. Taken together, it could be speculated that cancer cells in HCC patients with GALNT14-rs9679162 “GG” genotype are more sensitive to ICIs therapy. The expression of GALNT14 may be influenced by SNP GALNT14-rs9679162 via the potential underlying mechanisms mentioned above, resulting in increased sensitivity to ICIs therapy in HCC patients. The functional roles of the SNP GALNT14-rs9679162/GALNT14 expression/ICIs response axis in HCC need to be determined in the future.
The adverse effects of ICIs are generally mild, with approximately 10% of patients experiencing severe grade 3-4 events [6]. Nevertheless, these inhibitors, such as CTLA-4 and PD-(L) 1 inhibitors, typically result in an increase in side effects, including elevated levels of AST [18, 20]. Histologically, ICIs can lead to conditions like granulomatous hepatitis with fibrin deposition/central vein endotheliitis [20] or lobular non-granulomatous hepatitis [18]. Notably, post-treatment AST-related liver dysfunction has been linked to poorer PFS in patients with advanced cancer following ICI (nivolumab or pembrolizumab) monotherapy [21]. In our HBV-infected HCC patients receiving ICI (atezolizumab plus bevazizumab) therapy, it showed that post-treatment AST with a high grade was associated with a shorter PFS. More importantly, our data further demonstrated that the GALNT14-rs9679162 “GG” genotype was associated with a decreased risk of post-treatment AST with a high grade when compared with GALNT14-rs9679162 “non-GG” genotype. After stratifying by post-treatment AST grade, GALNT14-rs9679162 “GG” genotype associated with a decreased risk of post-treatment disease progression was only observed in subgroups with low post-treatment AST grade but not in subgroups with high post-treatment AST grade. According to these findings, it implicates that patient with GALNT14-rs9679162 “GG” genotype is more susceptible to ICI therapy, which might also reduce the occurrence of these side effects to further influence the post-treatment disease progression. For this aspect, we thus recommended that ICI therapy may be a suitable option for treating HCC patients with GALNT14-rs9679162 “GG” genotype. Moreover, post-treatment monitoring for AST-related side effect in HCC patients treated with ICI is necessary in the following follow-up.
The gene GALNT14, situated on chromosome 2, is a member of the polypeptide N-acetylgalactosaminyltransferase family. This family is involved in catalyzing protein O-glycosylation, and dysregulated GALNT expression has been linked to altered O-glycosylation patterns in various cancers [22, 23]. Even though not much is known about how GALNT14 works in HCC, studies have shown that it helps cells divide and move around, and that blocking it makes cells more sensitive to anticancer drugs [10]. Recently, Li et al. [9] have proposed that the downregulation of GALNT14 may induce ferroptosis by inhibiting the mTOR/EGFR pathway, subsequently reducing the protein levels of SLC7A11 and GPX4. Inhibition of ferroptosis has been associated with decreased AST levels and improved survival in drug-induced liver injuries [24]. Teraoka [25] suggests that the unidentified immune activity in the tumor may enhanced the effect of ICI in the early phase, which results in liver injury due to T cell recognition and activity against antigens in healthy tissues. Based on the results of these findings and the present study, we speculated that SNP GALNT14-rs9679162 may influence the post-ICI PFS in HCC patients via GALNT14 expression-regulated ferroptosis/AST/liver injury axis. To provide improving treatment with ICIs and important clues on the mechanism of ICI-mediated toxicity and antitumor efficacy, further investigation is required to elucidate the mechanisms driving these associations.
Currently, age has not been utilized as a stratification variable that could influence safety and complications in the large-scale clinical trials of ICIs for HCC [26]. However, adverse events (AE) and efficacy of immunotherapy in the older population may differ from those in younger patients [26]. Compared to these findings, we noted that older age was associated with a decreased risk of post-treatment disease progression in HCC patients following ICI. Furthermore, this association was only observed in subgroups with high post-treatment AST grade but not in subgroups with low post-treatment AST grade, indicating that older age and severe post-treatment AST-related side effect could have a synergistic effect to reduce the risk of post-treatment disease progression. Mechanistically, a possible explanation is that older patients have a higher incidence of all-grade AEs after ICI therapy [27]. Patients who experience a higher grade AE should have a higher T-cell activity and, hence, experience better antitumor outcomes than patients who experience a lower grade AE [28].
HCC patients with lower ALBI grades had better response to immunotherapy and prognosis [29]. Similarly, the results of the present study also exhibited that an elevated ALBI grade (III + IV) was associated with an increased risk of post-treatment disease progression in HCC patients with ICI. Of note, we further demonstrated that this association was only observed in subgroups with high post-treatment AST grade but not in subgroups with low post-treatment AST grade, indicating that elevated ALBI grade and severe post-treatment AST-related side effect (liver dysfunction-related side effect) could have a synergistic effect to enhance the risk of post-treatment disease progression. For this finding, it may be because cirrhosis is the common concomitant liver disease in HCC patients, and an elevated ALBI grade is indicative of deteriorating liver function and more advanced cirrhosis [30]. The presence of cirrhosis can facilitate tumor immune evasion and foster an immunosuppressive microenvironment. For instance, cirrhotic livers exhibit increased levels of extracellular matrix components, which can further inhibit anti-tumor immunity through the activation of transforming growth factor (TGF)-β [31]. Moreover, liver fibrogenesis is stimulated by hepatic stellate cells, which may reduce lymphocyte infiltration and promote the proliferation of immunosuppressive cells [32].
The present retrospective study has several limitations. First, all patients were recruited from the same hospital and data were retrospective, which together may result in selection bias. Also, cross-sectional, observational study does not allow inferences of causality. Secondly, the sample size of the present study was relatively small, and further studies with a larger population are needed to verify the present findings. Lastly, the molecular mechanisms underlying the survival-associated SNP rs6752303/AST grade axis and the observed association call for direct biological experiments and future prospective study for functional validation.
Conclusion
The present study identified a significant association between SNP GALNT14-rs9679162 and survival of HBV-related HCC patients received ICI therapy. The protective genotypes of this SNP may contribute to a better post-treatment PFS in an AST-mediated manner. These results may provide clinicians with some valuable information for risk stratification and treatment strategy development in the care of patients with HBV-related HCC undergoing ICIs therapy.
Abbreviations
AST: aspartate aminotransferase
DCR: disease control rate
HCC: hepatocellular carcinoma
HFSR: hand-foot skin reaction
ICIs: immune checkpoint inhibitors
ORR: objective response rate
OS: overall survival
PFS: progression-free survival
SNP: single nucleotide polymorphism
Supplementary Material
Supplementary tables.
Acknowledgements
The authors thank all the members of the Cancer Center, Chang Gung Memorial Hospital, for their invaluable help including patient recruitment, data collection, and clinical follow-up. The authors also appreciate for their assistance in data analysis. The authors are also grateful to the Lin Huang Yueh-Ying Medical Foundation for their academic guidance and support.
Funding
Grants from Chang Gung Medical Research Fund (CMRPG3Q0011), Chang Gung Memorial Hospital (CORPG3P0411), NSTC 112-2314-B-182A-016-MY3, and National Science Council, Taiwan (NMRP- G3N6011).
Competing Interests
The authors have declared that no competing interest exists.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A. et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71:209-49
2. Forner A, Da Fonseca LG, Diaz-Gonzalez A, Sanduzzi-Zamparelli M, Reig M, Bruix J. Controversies in the management of hepatocellular carcinoma. JHEP Rep. 2019;1:17-29
3. Chen DS, Hurwitz H. Combinations of Bevacizumab with Cancer Immunotherapy. Cancer J. 2018;24:193-204
4. Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY. et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med. 2020;382:1894-905
5. Ding X, He M, Chan AWH, Song QX, Sze SC, Chen H. et al. Genomic and Epigenomic Features of Primary and Recurrent Hepatocellular Carcinomas. Gastroenterology. 2019;157:1630-45 e6
6. Nadeau BA, Fecher LA, Owens SR, Razumilava N. Liver Toxicity with Cancer Checkpoint Inhibitor Therapy. Semin Liver Dis. 2018;38:366-78
7. Yeh CT, Liang KH, Lin CC, Chang ML, Hsu CL, Hung CF. A single nucleotide polymorphism on the GALNT14 gene as an effective predictor of response to chemotherapy in advanced hepatocellular carcinoma. Int J Cancer. 2014;134:1214-24
8. Lin CL, Chien RN, Chen LW, Chu YD, Yeh CT. Rs9679162 genotype predicts prognosis of real-world advanced hepatocellular carcinoma treated by sorafenib. Cancer Biomark. 2023;36:251-66
9. Chu YD, Liu HF, Chen YC, Chou CH, Yeh CT. WWOX-rs13338697 genotype predicts therapeutic efficacy of ADI-PEG 20 for patients with advanced hepatocellular carcinoma. Front Oncol. 2022;12:996820
10. Chu YD, Fan TC, Lai MW, Yeh CT. GALNT14-mediated O-glycosylation on PHB2 serine-161 enhances cell growth, migration and drug resistance by activating IGF1R cascade in hepatoma cells. Cell Death Dis. 2022;13:956
11. Chu YD, Ho PH, Chen WT, Shih YL, Lai MW, Hsu CW. et al. GALNT14 Genetic Variants Harbor Differential Prognostic Values Linking to Distinct Macrophage Cell Types in Hepatocellular Carcinoma. J Hepatocell Carcinoma. 2025;12:1695-710
12. Jin Y, Jin C, Xie R, Zhang J, Wei G, Zheng L. HBV reactivation during immunotherapy for hepatocellular carcinoma: risk factors and clinical management. Front Immunol. 2026;17:1765054
13. Bolondi L, Burroughs A, Dufour JF, Galle PR, Mazzaferro V, Piscaglia F. et al. Heterogeneity of patients with intermediate (BCLC B) Hepatocellular Carcinoma: proposal for a subclassification to facilitate treatment decisions. Semin Liver Dis. 2012;32:348-59
14. Kim JH, Shim JH, Lee HC, Sung KB, Ko HK, Ko GY. et al. New intermediate-stage subclassification for patients with hepatocellular carcinoma treated with transarterial chemoembolization. Liver Int. 2017;37:1861-8
15. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R. et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228-47
16. Sznol M. Reporting disease control rates or clinical benefit rates in early clinical trials of anticancer agents: useful endpoint or hype? Curr Opin Investig Drugs. 2010;11:1340-1
17. Liang KH, Yang PC, Yeh CT. Genotyping the GALNT14 gene by joint analysis of two linked single nucleotide polymorphisms using liver tissues for clinical and geographical comparisons. Oncol Lett. 2014;8:2215-20
18. De Martin E, Michot JM, Papouin B, Champiat S, Mateus C, Lambotte O. et al. Characterization of liver injury induced by cancer immunotherapy using immune checkpoint inhibitors. J Hepatol. 2018;68:1181-90
19. Liu Y, Liu H, Yang L, Wu Q, Liu W, Fu Q. et al. Loss of N-Acetylgalactosaminyltransferase-4 Orchestrates Oncogenic MicroRNA-9 in Hepatocellular Carcinoma. J Biol Chem. 2017;292:3186-200
20. Tian Y, Abu-Sbeih H, Wang Y. Immune Checkpoint Inhibitors-Induced Hepatitis. Adv Exp Med Biol. 2018;995:159-64
21. Yokohama K, Asai A, Matsui M, Okamoto N, Yasuoka H, Nishikawa T. et al. Liver dysfunction is associated with poor prognosis in patients after immune checkpoint inhibitor therapy. Sci Rep. 2020;10:14470
22. Bennett EP, Mandel U, Clausen H, Gerken TA, Fritz TA, Tabak LA. Control of mucin-type O-glycosylation: a classification of the polypeptide GalNAc-transferase gene family. Glycobiology. 2012;22:736-56
23. Beaman EM, Brooks SA. The extended ppGalNAc-T family and their functional involvement in the metastatic cascade. Histol Histopathol. 2014;29:293-304
24. Yamada N, Karasawa T, Kimura H, Watanabe S, Komada T, Kamata R. et al. Ferroptosis driven by radical oxidation of n-6 polyunsaturated fatty acids mediates acetaminophen-induced acute liver failure. Cell Death Dis. 2020;11:144
25. Teraoka S, Fujimoto D, Morimoto T, Kawachi H, Ito M, Sato Y. et al. Early Immune-Related Adverse Events and Association with Outcome in Advanced Non-Small Cell Lung Cancer Patients Treated with Nivolumab: A Prospective Cohort Study. J Thorac Oncol. 2017;12:1798-805
26. Lyu N, Yi JZ, Zhao M. Immunotherapy in older patients with hepatocellular carcinoma. Eur J Cancer. 2022;162:76-98
27. Ng KYY, Tan SH, Tan JJE, Tay DSH, Lee AWX, Ang AJS. et al. Impact of Immune-Related Adverse Events on Efficacy of Immune Checkpoint Inhibitors in Patients with Advanced Hepatocellular Carcinoma. Liver Cancer. 2022;11:9-21
28. Passat T, Touchefeu Y, Gervois N, Jarry A, Bossard C, Bennouna J. [Physiopathological mechanisms of immune-related adverse events induced by anti-CTLA-4, anti-PD-1 and anti-PD-L1 antibodies in cancer treatment]. Bull Cancer. 2018;105:1033-41
29. Wong JSL, Kwok GGW, Tang V, Li BCW, Leung R, Chiu J. et al. Ipilimumab and nivolumab/pembrolizumab in advanced hepatocellular carcinoma refractory to prior immune checkpoint inhibitors. J Immunother Cancer. 2021 9
30. Johnson PJ, Berhane S, Kagebayashi C, Satomura S, Teng M, Reeves HL. et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol. 2015;33:550-8
31. Henderson NC, Arnold TD, Katamura Y, Giacomini MM, Rodriguez JD, McCarty JH. et al. Targeting of alphav integrin identifies a core molecular pathway that regulates fibrosis in several organs. Nat Med. 2013;19:1617-24
32. Affo S, Yu LX, Schwabe RF. The Role of Cancer-Associated Fibroblasts and Fibrosis in Liver Cancer. Annu Rev Pathol. 2017;12:153-86
Author contact
![]() Corresponding authors: Chun-Yen Lin, MD, PhD, Professor, Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou branch, No. 5, Fuxing St., Guishan Dist., Taoyuan City, 333, Taiwan, Tel: 886-3-3281200 ext. 8120, Fax: 886-3-3282824, Email: chunyenlincom. Chau-Ting Yeh, MD, PhD, Liver Research Center, Linkou Chang Gung Memorial Hospital, No. 5, Fuxing St., Guishan Dist., Taoyuan City, 333, Taiwan, Tel: 886-3-3281200 ext. 8120, Fax: 886-3-3282824, Email: chautingycom.
Corresponding authors: Chun-Yen Lin, MD, PhD, Professor, Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou branch, No. 5, Fuxing St., Guishan Dist., Taoyuan City, 333, Taiwan, Tel: 886-3-3281200 ext. 8120, Fax: 886-3-3282824, Email: chunyenlincom. Chau-Ting Yeh, MD, PhD, Liver Research Center, Linkou Chang Gung Memorial Hospital, No. 5, Fuxing St., Guishan Dist., Taoyuan City, 333, Taiwan, Tel: 886-3-3281200 ext. 8120, Fax: 886-3-3282824, Email: chautingycom.